Lung disease is a common cause of morbidity and mortality in patients with rheumatoid arthritis (RA). Currently, there are no screening guidelines for parenchymal lung diseases (interstitial lung disease [ILD] and emphysema) in RA.
In a prospective study, Jeffrey A. Sparks, MD, MMSc, of the Division of Rheumatology, Inflammation, and Immunity, and senior/corresponding author Tracy J. Doyle, MD, of the Division of Pulmonary and Critical Care Medicine, both at Brigham and Women’s Hospital; and Anthony J. Esposito, MD, previously at the Brigham and now at Northwestern Feinberg School of Medicine, and colleagues identified a high prevalence of undiagnosed preclinical parenchymal lung disease in an RA cohort. The finding was driven primarily by isolated emphysema, which was common even in never-smokers. In Rheumatology (Oxford) the researchers discuss important implications of their findings.
Methods
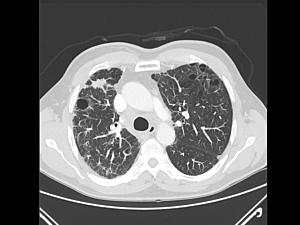
Between November 2016 and December 2019, the researchers enrolled 106 patients with RA who did not have a history of ILD, emphysema or chronic obstructive pulmonary disease. All patients underwent a physical examination, high-resolution computed tomography (HRCT) of the chest, pulmonary function tests, six-minute walk test, blood testing and completed symptom questionnaires.
Prevalence of Parenchymal Lung Diseases
Imaging identified preclinical emphysema and/or preclinical ILD in 48 patients (45%). Compared to RA patients without parenchymal lung disease, these patients:
- Were significantly older
- Had a lower percent predicted diffusing capacity of the lung for carbon monoxide (%DLCO)
- Were similar with regard to sex, smoking, RA duration, current RA activity and current/ever use of immunosuppressive therapy, spirometry results and dyspnea rates
The prevalence of preclinical ILD (16 patients, 15%), was lower than previously reported and not associated with any demographic, functional, or symptomatic measures when compared with individuals without preclinical ILD.
The Emphysema Subgroup
The high prevalence of parenchymal lung disease was driven by emphysema (38 patients, 36%). Compared to RA patients without emphysema, these patients:
- Had significantly higher cyclic citrullinated peptide titers
- Were more likely to have a diffusion defect
- Were more likely to have bronchiectasis
- Were similar with regard to sex, smoking history, RA characteristics and immunosuppressive medications
Patients with moderate/severe emphysema were more likely to have a cough. This is the first study of isolated emphysema in the general RA population.
Preclinical Emphysema and Smoking Status
18 of the patients with preclinical emphysema were never-smokers. Thus, never-smokers represented 47% of RA patients with preclinical emphysema and, stated differently, 31% of never-smokers with RA had preclinical emphysema.
Never-smokers with emphysema were younger and had a higher %DLCO than ever-smokers with emphysema. In addition, their HRCT scans showed a higher proportion of panlobular distribution, which may be associated with immune etiologies (published in European Respiratory Journal). Ever-smokers were more likely to have the classic smoking-related centrilobular distribution. These differences suggest RA may be an independent risk factor for emphysema.
Considerations for Clinicians
There is an unmet need in RA for early detection of preclinical parenchymal lung disease. Both ILD and emphysema are significant public health problems, and interventions are available that are potentially more effective before respiratory symptoms develop.
It is unknown when a patient with preclinical emphysema becomes symptomatic or has an increased risk of disease progression or complications, but it’s noteworthy that some of the individuals in this study with emphysema were already symptomatic and functionally impaired at the time of imaging.
Furthermore, this study demonstrates preclinical ILD can’t be reliably identified by symptoms, physical exam, or laboratory or pulmonary function tests. High-resolution CT may be the only reliable clinical screening tool currently available.
Smoking cessation remains a vital aspect of caring for all patients with RA. It is a well-documented risk factor for emphysema and ILD and has been tied to increased RA disease activity.
Further studies are required to establish the clinical significance of these preclinical parenchymal abnormalities, to determine the optimal approach to detect undiagnosed disease, and to characterize the subset of patients who progress and may benefit from early intervention.